


UKHSA's failure on airborne transmission and a Vax only strategy without Vax
Recent guidance, Airborne transmission dismissed at Covid Inquiry, removal of vax and the dismantling of public health,

With the UK's NHS currently under extreme pressure from what has been labelled a “quad-demic” of respiratory illnesses, the UK Health Security Agency (UKHSA) is facing criticism from experts in public health regarding its guidance for cutting transmission which ignores reducing airborne transmission, instead focusing on handwashing.
The guidance resembles what was produced in early 2020, however public health advice hasn’t been stagnant for five years in the UK, it took a step forward a few years ago with messaging on ventilation and covid lingering in the air, then unfortunately public health took a step back with this messaging disappearing.
The UK has returned to the same messaging it had at the start of the pandemic when the plan was to manage Covid's passage through the population. This is because the UK has adapted the original herd immunity strategy to one of regular repeated mass infection. Unlike in many other countries, covid vaccines were only seen by the UK as a short term initiative to allow a return to normal. This is why the UK has been gradually withdrawing access to vaccines.
How has public health in the UK manage to regress? Many of those involved in originally downgrading PPE guidance for healthcare workers are still in senior public health positions.
In the Covid Inquiry’s third module on the impact of the pandemic on healthcare systems, the chair Baroness Hallet had an opportunity to examine the Four Nations Infection Prevention Control (IPC) Cell’s decision making with key individuals giving testimonies including Dr Lisa Richie who chaired the cell through the second wave.
In August 2023 the Byline Times published an exclusive investigation into the timeline of key decisions that led to healthcare workers outside of specific settings wearing loose surgical masks rather than high quality fit tested respirators known as FFP3s. This included the controversial decision on 13 March 2020 to downgrade covid from being a High Consequence Infectious Disease (HCID), at a time when there was a crisis in PPE supply, which led to healthcare workers accusing the government of failing to protect them from preventable harms and death.
However the timeline had gaps due to the secretive nature of the IPC Cell which executed a “command role” during the national management of Covid, steering the NHS and coordinating decisions UK-wide. Minutes were taken, but unlike other key committees like SAGE they were never released into the public domain. Only a few sets of meeting minutes obtained through Freedom of Information requests (FOI) from the height of the second wave have become public. These show that while Public Health England (PHE) recommended a much wider use of respirator FFP3 masks, the IPC cell rejected this.
After hearing analysis from a series of experts including Dr Barry Jones of the Covid Airborne Transmission Alliance (CATA) that the health authorities’ assumption covid was transmitted by large short range droplets rather than smaller long range aerosols was in Jones’ words “dishonest and wrong”, key figures from the Infection Prevention Control (IPC) Cell, Royal College of Nursing (RCN) and Public Health England (PHE); now UKHSA, failed to provide convincing answers to simple questions regarding aerosol transmission and the use of FFP3s. This culminated with Hallet’s own incredulous reaction when she held up a fit tested respirator and a flimsy surgical mask in response to Professor Susan Hopkin of PHE’s assertion there was weak evidence of any difference in effectiveness between the two.
The testimonies of these individuals received fierce criticism from core participants for Module Three and members of the scientific community around the world. Dr David Tomlinson; a member of CATA, said that while he believed there was never going to be an apology for the IPC guidance that drove disproportionately high rates of death and covid in non ICU healthcare workers “the level of obfuscation,evasion and incompetence on display from those tasked with keeping healthcare workers safe, is jaw dropping.”
For example speakers from government agencies failed to agree who was ultimately responsible for IPC guidance. Richie; IPC Cell said the senior clinicians group was responsible, Ruth May; senior clinicians group and Senior Responsible Officer for the IPC Cell, said it was PHE ,while Hopkins; PHE said it was the IPC Cell. CMO Chris Whitty; also in the senior clinicians group, said “There were too many people with partial responsibility.”
IPC guidance was based on the ‘consensus’ of IPC Cell members, however no formal votes were ever taken, Richie as chair summarised what she believed to be the consensus.
The group Clinically Vulnerable Families; core participants, highlighted the IPC Cell's contradictory approach to evidence. “Outdated views on droplet sizes from 1997 were considered more credible than evidence from expert physical scientists”, while more recent SARS evidence “appeared to have been partly dismissed for being from 10 years ago". The failure to learn from SARS was identified in Hallet’s module one report, and she questioned the cell’s conclusions by quoting SARS guidance from 2013 recommending FFP3s that Richie co-authored alongside Professor Jonathan Van-Tam.
Richie explained the decision to recommend surgical masks was based on knowledge of SARS and the WHO’s initial declaration that “covid is not airborne”, which is widely considered to be a catastrophic error. Richie stated that while she now believed “airborne spread is possible” it’s not the predominant route “and, indeed, the WHO guidance has not stated a change in a predominant mode of transmission for SARS-CoV-2.”
The WHO did initially state covid was spread via droplets, however the guidance was updated to say aerosols and droplets are the main mode of transmission. Hopkins in her testimony agreed with Richie on aerosols, however independent expert witnesses who appeared earlier in the inquiry had provided evidence demonstrating why aerosols are the primary mode, and that a strong evidence base had been established by summer 2020.
When asked whether the fact doctors wearing higher quality PPE were dying at lower rates & were infected at lower rates indicated that it was necessary to spread the use of higher quality PPE more widely to other areas Richie replied “No.”
Ritchie also said patients should never wear FFP3 masks because valved masks ‘leak’ out infectious particles, neglecting the fact standard hospital FFP3s don’t have valves.
The module has continuing relevance as guidance for healthcare settings still doesn’t focus on mitigations against aerosols such as ventilation, air filtration or respirators with examples of clinically vulnerable patients being told to remove their high grade masks despite hospital acquired infections placing a considerable but preventable burden on the NHS.
When asked whether there was ever a point when the cell collectively thought airborne transmission was a significant threat requiring FFP3s, Ritchie responded “No.”
Johnson’s former political advisor Dominic Cummings responded to Richie's testimony on social media by saying “The system is working as intended” stating that “in 2020 I said the official slogan should change to include VENTILATE. This never happened.” Continuing “one of the weirdest most interesting things on covid is the extreme resistance across bureaucracies to accepting it was mainly airborne.”
An extract from the September 2020 IPC Minutes provides a possible reason for the reticence to change position on FFP3s, “If you wanted to change the guidance itself, it would need a very careful narrative as it would be easy to give the impression that we got it wrong the first time.”
The failure to recognise the importance of clean air and respirators in cutting transmission was repeated by a succession of other individuals in government public health positions.
The question is, how have they've managed to maintain their positions, both in terms of the science and employment?
Is it a matter of ideology, a refusal to admit mistakes, or could it be that they've stopped looking at the evidence because they're not longer concerned with reducing transmission?
Professor Susan Hopkins, UKHSA's Chief Medical Advisor who told the inquiry masks don't work and aerosols aren't the main mode of transmission was asked in an interview in September 2023 why the booster was restricted to a narrow range of groups. Her response was that most people had a good level of immunity, when it was highlighted that many people hadn't had a booster for more than a year, she replied that coming into contact with covid would boost immunity.
It would appear that when Public Health England changed to UKHSA, the purpose of preventing infectious disease changed to one of simply managing disease.
Living with Covid
The UK government produced a Living with Covid Strategy in 2022 which: against the evidence, declared covid to have become endemic and set out what was effectively a vax only strategy.
The JCVI appear to agree with this strategy as primary vaccination has been discontinued and eligibility for boosters is increasingly narrow, with future boosters set to exclude previously at risk groups such as pregnant women.
Calculations for the benefit of vaccination only take into account hospitalisations and deaths, long covid and economic impact of both short and long term sickness are not considered by the JCVI, or seemingly the UKHSA.
https://bylinetimes.com/2024/12/09/covid-vaccines-at-risk-jcvi/
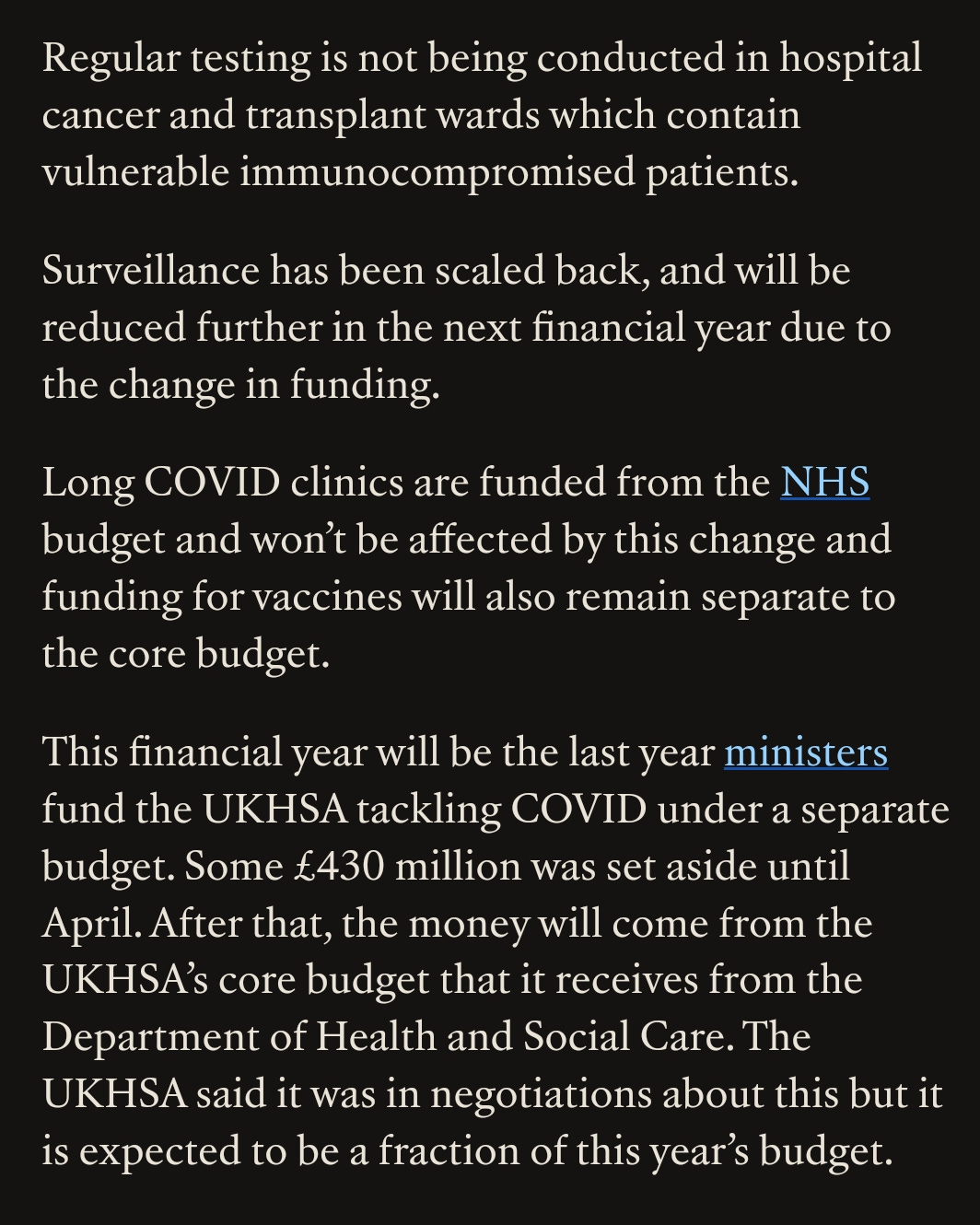
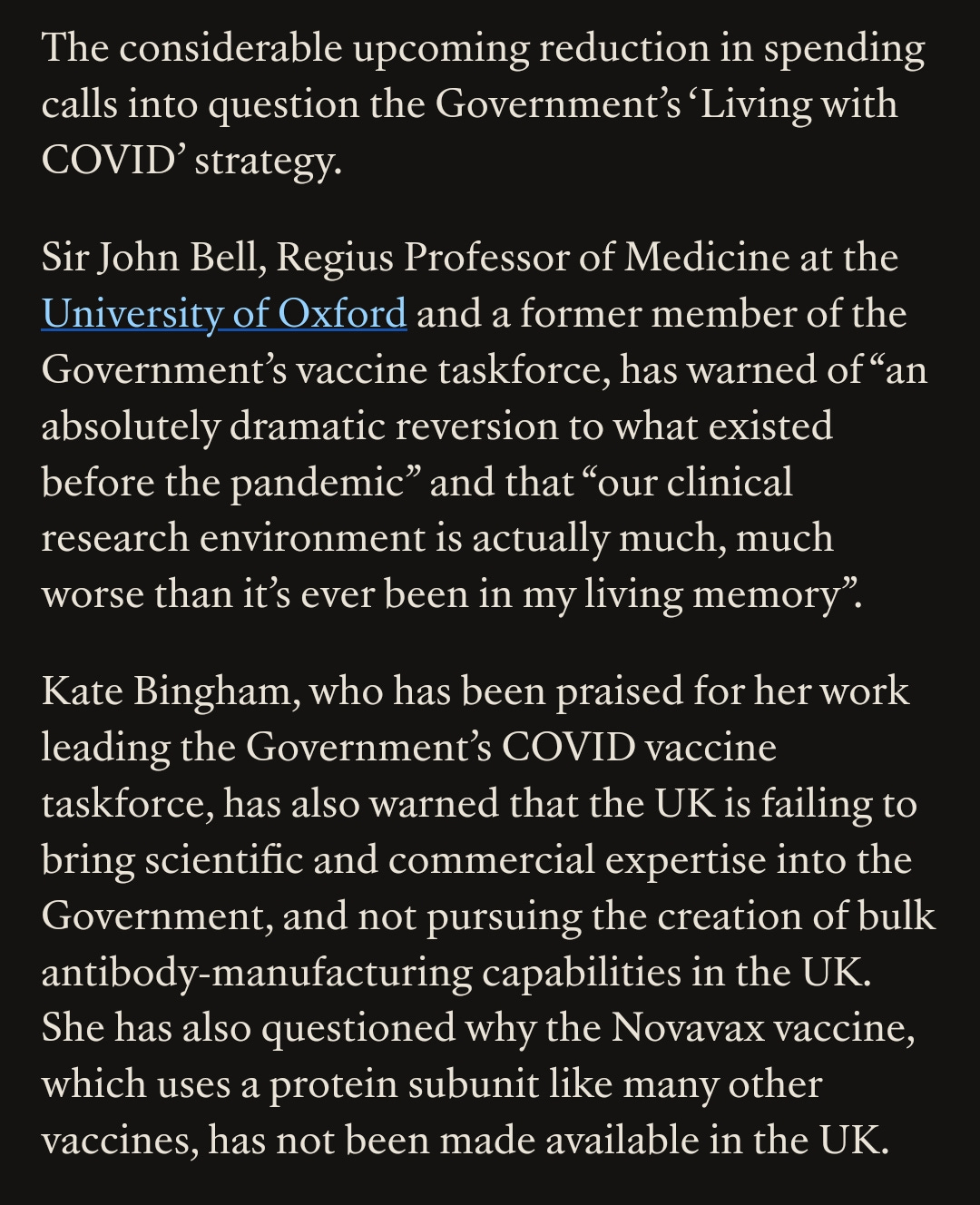
The previous Conservative Government didn't keep to its own Living with Covid strategy document, rather than learning from previous mistakes they proceeded to end.Covid funding and dismantledthe infrastructure of surveillance and the means to respond to the emergence of a more pathogenic variant.
From a year ago.
https://bylinetimes.com/2024/01/03/government-phases-out-covid-funding-as-hospital-admissions-rise/
Rather than ending up in a stronger position to face pandemics, the UK finds itself at best back at square one, if not in a worse position.
A number of hospitals have reintroduced masks in all departments. Also soap and water is better than any hand gel, particularly since norovirus is unaffected by alcohol gel. If I wear a mask, that doesn’t protect me from you, but it does protect you from me. The problem is that you can be infected and contagious up to 24 hours before you develop symptoms, as the incubation period is of the same order as the innate immune response (those first symptoms are actually due to your immune response). The other issue is that the vaccines cannot prevent you becoming infected neither can they prevent you from being infectious.
I would suggest that pregnant women are not at risk themselves, but their newborn will be. Pregnant women are vaccinated against pertussis and now RSV in the third trimester to provide passive antibody protection to the baby. Any neonate is at high risk from all respiratory tract infections, however preterm babies are at a significantly higher risk as their airways are very narrow. Their innate immune system is also likely to be underdeveloped.