
The Blame Game Part 2: Government Advisers
Examining the causes of vax hesitancy in parents

Part I examining claims the “myopic pro-vax eulogising” roll out of covid vax to children is the cause of polio outbreaks can be found here.

Pre-empting the JCVI
In the summer of 2021 while the JCVI were considering if they would recommend covid vaccination for ages 12-15, independent polling found that 90% of parents wanted to have their children vaccinated. Millions of teenagers had already been vaccinated in other countries when the JCVI initially decided to delay their decision, before then choosing not to recommend vaccination.
Prior to the decision those who would be presenting evidence to the JCVI on covid in children had made their opinions clear. These comments were seized on by anti-vax groups.

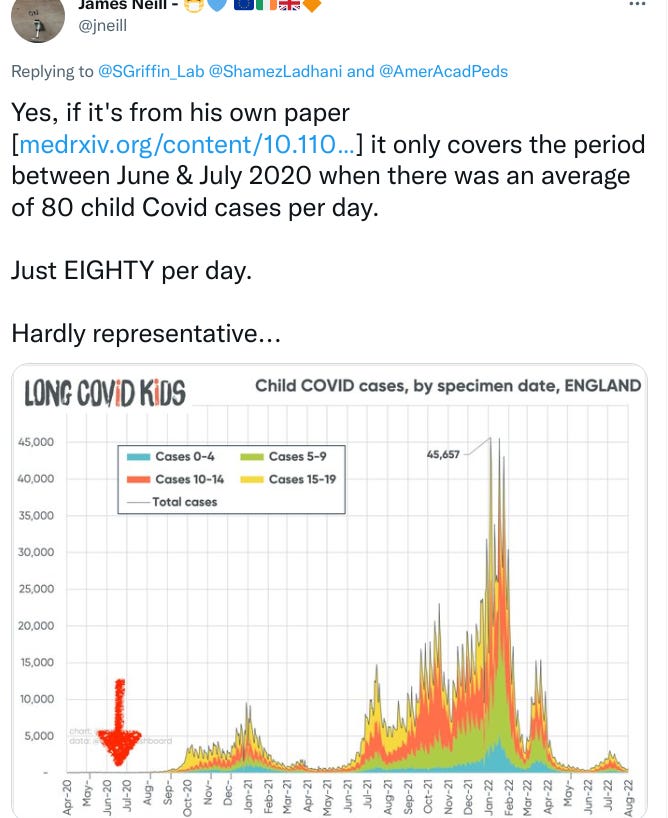
Ladhani’s studies are one of the main sources of evidence used by the UK Government to inform its decisions around schools and children.
Some professionals working with the UK Government decided to attack the US pediatric community to justify the stance in the UK.

The JCVI decision was based on their perception that the impact of covid on children was so low that the benefits of vaccination would be marginal. They accepted that without vaccination the majority of children would be infected with covid but considered natural immunity for children would be equal to vaccination.

This sounds like a herd immunity strategy for children.
However it’s now “depletion of susceptibles”.

Considering we are currently in a period where social media timelines are being flooded with anti-vax content, does advocating the benefits of natural immunity encourage or discourage parents vaccinating their children against other diseases?
Initially the JCVI approved 12-15 vaccination for those in certain at risk groups. Whilst the JCVI were still considering this, some of the messaging from the same individuals might have discouraged parents of the children most at risk from covid.

A detailed look at the minutes of the JCVI meetings where this was discussed can be found here


Negligible risk from covid?
Whether children should be vaccinated has mainly been defined by comparing risk from covid vs risk of vaccination. Some genuine hesitancy has been driven by minimising the harms of covid and exaggerating adverse reactions from vaccination.
Long covid in children is missing from the debate in the UK and elsewhere. The JCVI minutes show this was barely considered.


The ONS produces statistics on long covid in children.
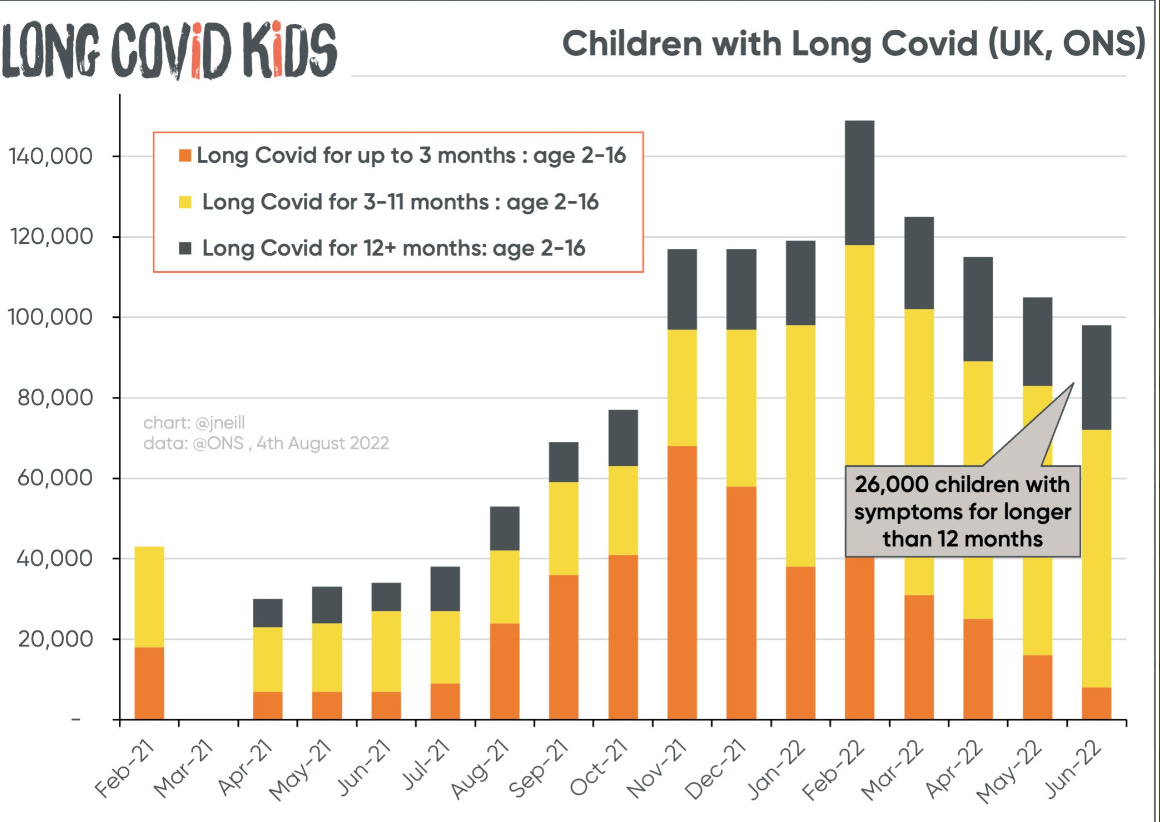
These inconvenient statistics and others with similar finding are not used to inform government policy, which relies almost entirely on a small group who rely on their own work. This is the same approach Sweden has taken.

5-11 Vax
The UK decided later than many other countries to approve vaccination for 5-11 year olds. The offer is “non urgent” meaning vaccines have been made available but aren’t being encouraged, this also means there won’t be any in school vaccination teams, inevitably leading to a lower take up as acknowledged by the JCVI. This is likely to reduce vaccination rates in certain communities and demographics more than others.
A decision has yet to be made in the UK regarding vaccination for children below five years of age.
Full JCVI minutes covering the 5-11 offer is here.
Encouraging?
It might be argued by some that in their apparent enthusiasm for the benefits of infection, professionals working with the UK Government have chosen messaging which has undermined confidence in covid vaccines for children. The friction between their comments and the decision to offer vaccination has created a space for anti-vax narratives to thrive.
It must be questioned if a fixation on herd immunity has influenced opposition to measures in schools.
A US perspective




