


Study examines UKs failure on airborne transmission
Care home deaths a consequence of expert certainty

After looking at the UKs pandemic response in schools the BMJ's covid inquiry series turns to the UKs resistance and inconsistent approach to airborne transmission
As with other analysis of the UK response the reliance on a small narrow group of advisers was highlighted.
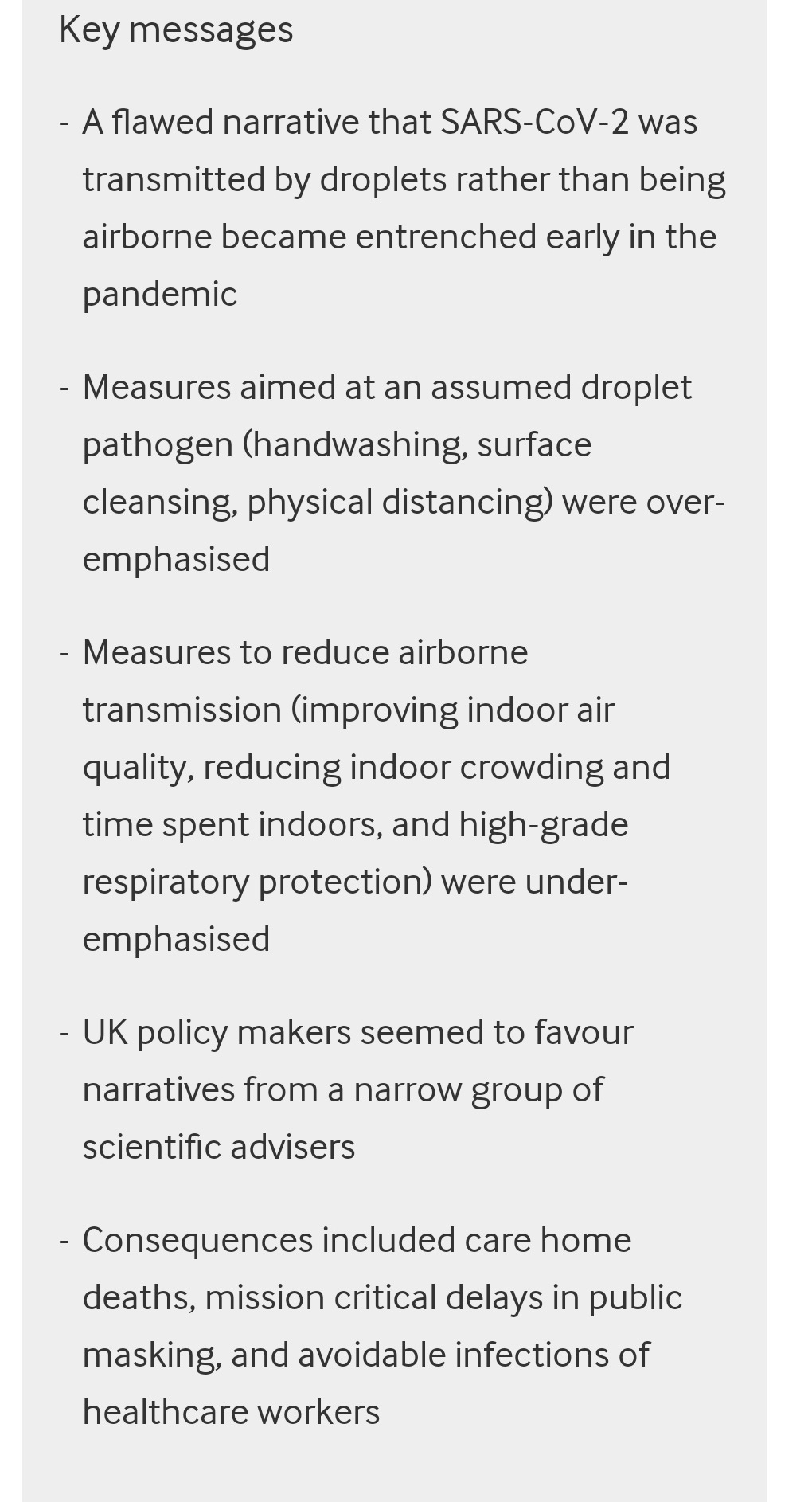
Flawed narratives around transmission led to misplaced policies and avoidable deaths.
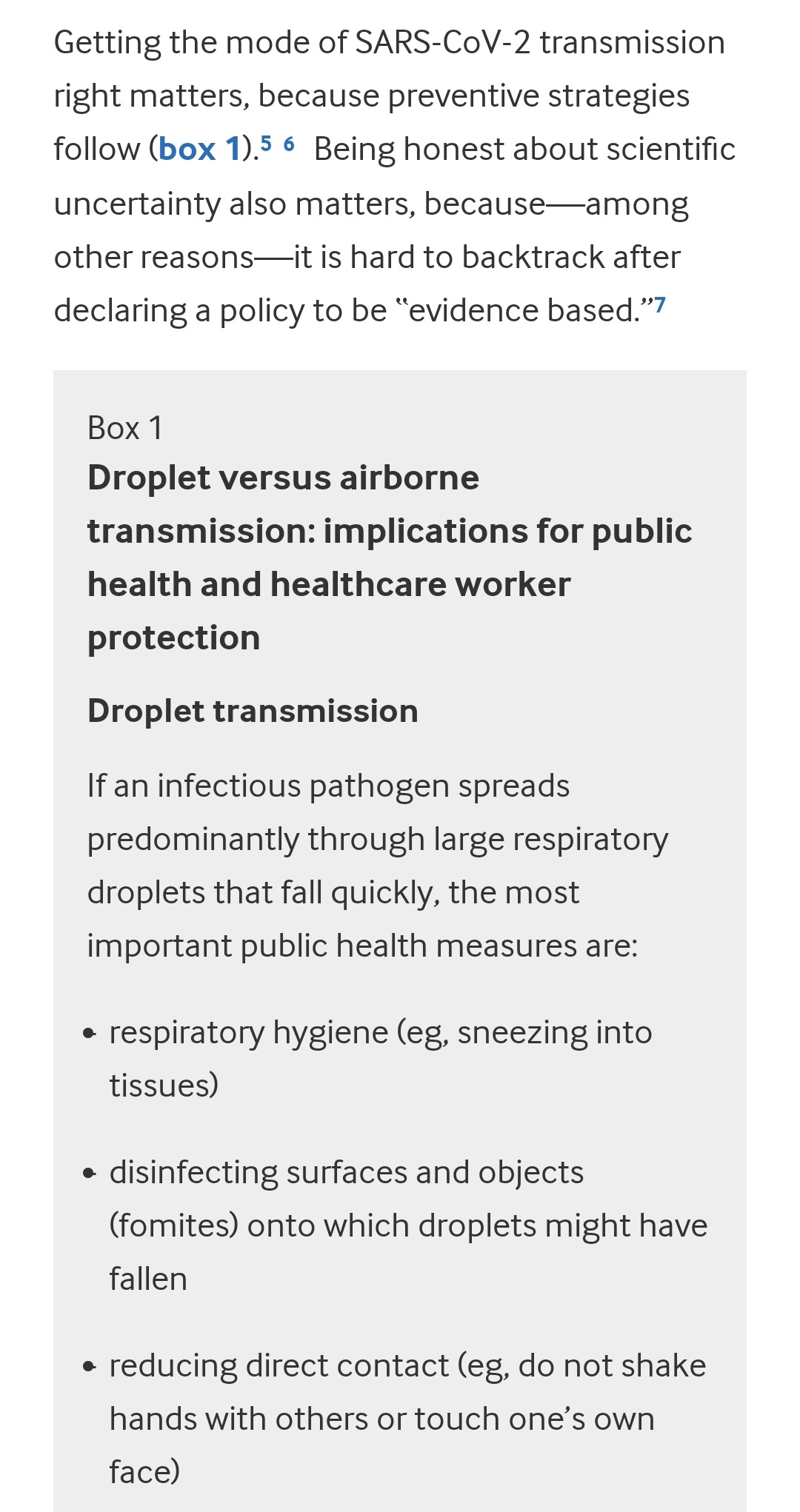
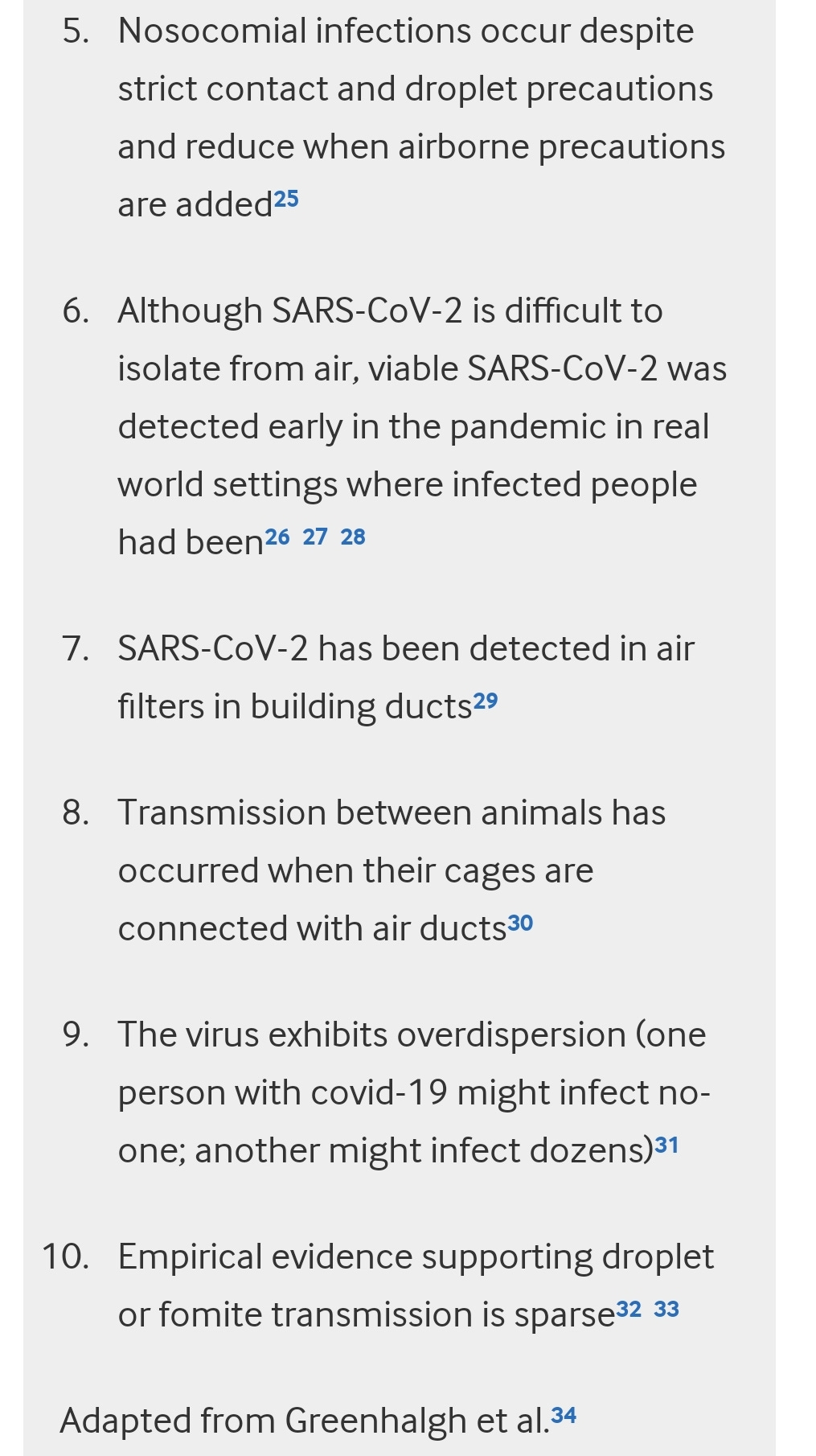
The study sets out the difference in policy between droplet and airborne transmission.
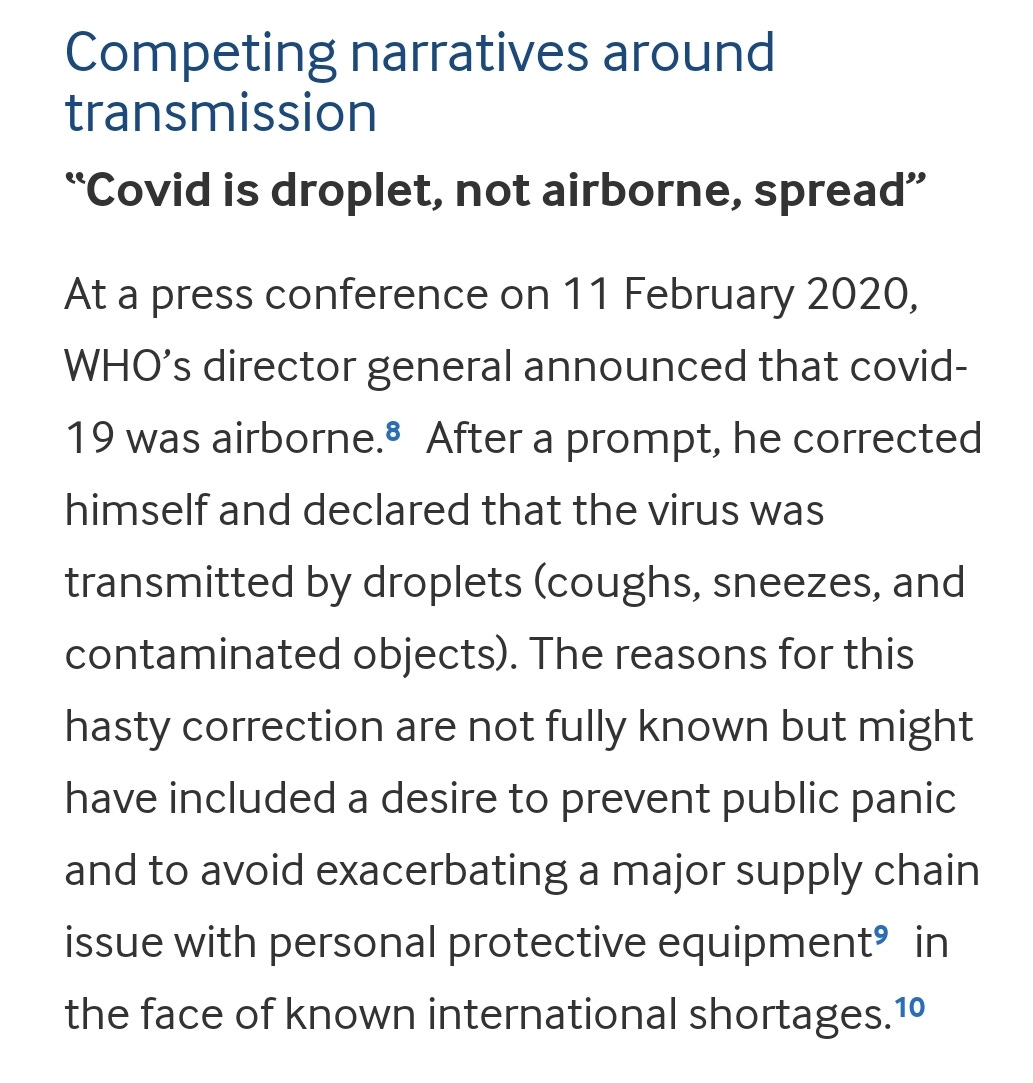
The confusion created by the infamous WHO press briefing on 11 February is highlighted.
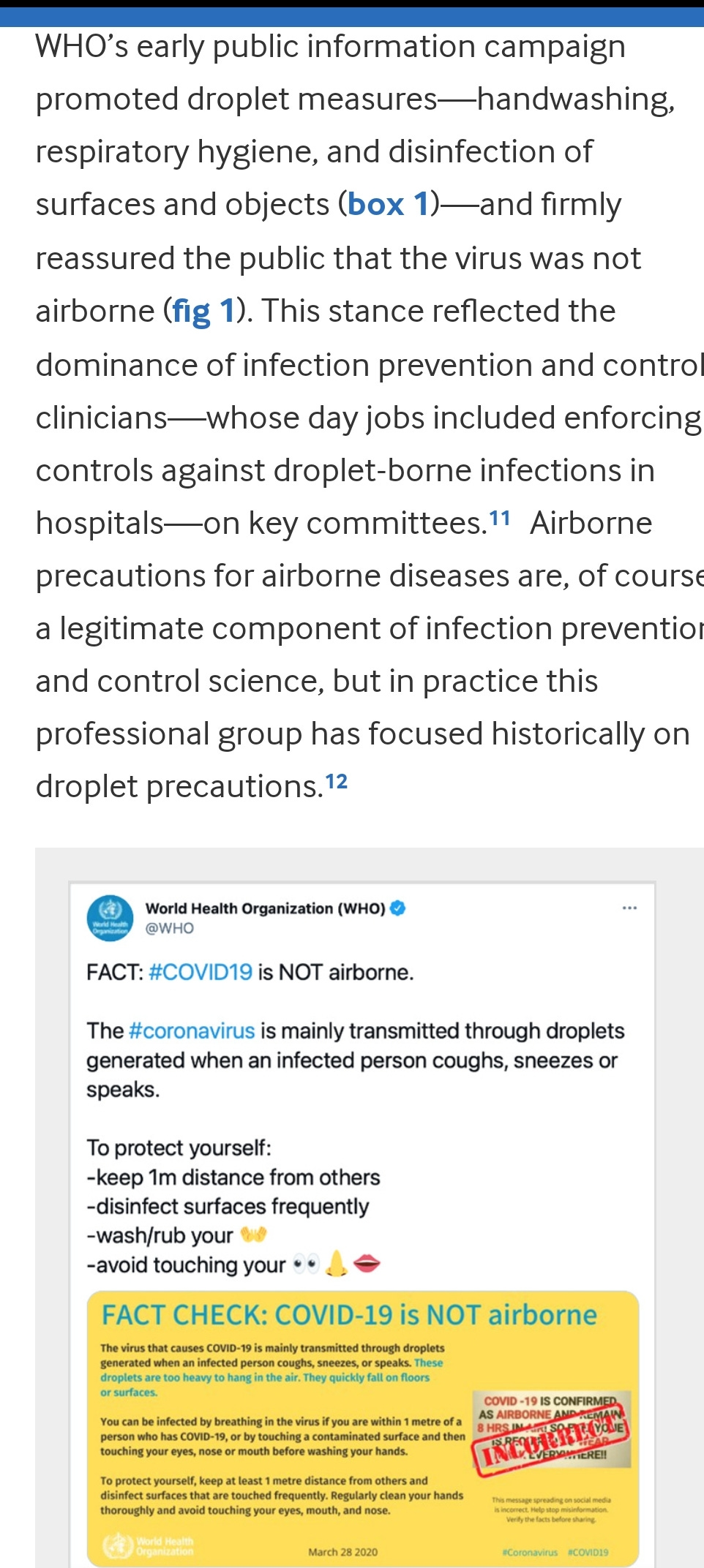
The failure to recognise airborne transmission by the WHO and the UK focusing on droplets led to hygiene theatre while masks and ventilation were ignored.
Counter Disinformation Project notes that denial of airborne transmission even though it had been raised in an early SAGE meeting would also support a strategy of mass infection. Of course it would be deeply unethical if a government were to claim measures were ineffective in order to facilitate mass infection.
The study's comparison of England vs Japan goes a long way to explaining how Japan with almost twice the population had 10% of the UKs death toll.
Failure to test patients discharged from hospitals combined with failure to mitigate against airborne transmission are cited as major factors in the decimation of care homes.
It should be noted those calling for focused protection also opposed mask wearing, dismissing a proven layer of mitigation does beg the question how care homes would have been protected whilst allowing high transmission.
The study provides Hong Kong as an example of where masks were part of a successful strategy to protect care homes in the first wave.
In January 2020 the UK government recognised asymptomatic transmission, however masks were only recommended for symptomatic cases. Masks were described as ineffective and potentially harmful due to contamination up to June 2020.
The effects of this confused early messaging still persists, particularly in regards to children, where contaminated masks as a mode of transmission is still cited as a reason not to recommend masks. Curiously professionals working with the UK government who have claimed there is no evidence of the effectiveness of masks in schools have also said their use could drag out the end of the pandemic by slowing down the build up of immunity. These are the same experts who also suggested infections in children were equivalent to a vaccine dose.
As we saw with transmission in children and schools there was a narrow definition of what evidence would be accepted. Lack of evidence was then interpreted by government and media as no evidence.
However NERVTAG minutes show serious concerns were raised regarding stockpiles of respirators, this is despite public reassurances that the UK was well prepared with adequate supply of PPE.
By early March 2020 the UK government had decided to follow a mass infection strategy in hope of achieving herd immunity, the measure for success was not directly preventing deaths, it was presenting the complete collapse of the NHS, the infamous Robert Peston article setting out this strategy was published in the Spectator on 12 March.
The decision to downgrade covid and therefore PPE requirements seems overly convenient considering shortages. At a similar time contact tracing had also been discontinued as the government was expecting the majority of the population to be infected.
Hypothesis
In early 2020 David Halpern who was advising the Cabinet Office on behalf of the Behavioural Insights Team spoke of “lockdown fatigue”. The term was widely criticised by behavioural scientists including other government advisers who didn’t know where the concept had come from. Could it be that policies makers simply didn’t believe the population would be willing to comply with lockdowns?
Its also possible that if a government had decided on a mass infection strategy then it would look for reasons not to introduce measures that would slow transmission. Halpern was the first person to speak of herd immunity in a media interview.
The second hypothesis is reminiscent of the paper on transmission in schools, a reliance on a narrow group of experts working with a selectively narrow evidence base.
The pandemic has shown the problems with gatekeeping by authorities, and of credentialism, from within government and the media.
The government reassured the public repeatedly that it was well prepared, when it became apparent they didn’t billions were spent on rushed PPE contracts which included a VIP lane for that was secret at the time.
Political ideology undoubtedly was opposed to lockdown, and so the concept of mass infection getting the pandemic over with quickly by achieving herd immunity would have appealed to the government.
The Counter Disinformation Project noted that with politicians making the decisions its impossible for politics to not enter the pandemic response. In 2021 internal party politics appears to have become a driving factor in government policy as the sceptic wing of the Conservative Party was large enough to overturn Johnson's parliamentary majority and relying on opposition votes would have earned the anger of Conservative supporting papers. Johnson was reliant on those papers to bolster his support as he attempted to withstand rolling scandals.
There was not enough PPE and the government didn’t want to create panic. There must have been discussions at some point regarding how frontline workers without appropriate PPE might react if the government stated covid was airborne.
What seems to have been forgotten by most is that the original lockdown was watered down within an hour or two.
Released with Johnsons speech, only key workers go to work.
Within two hours this had become work from home where possible.
What caused the change? Was it the difficulty in defining a key worker? Pressure from inside the party, donors or lobbying business interests? An attempt to keep up economic activity even though it increased the time it took for cases to fall?
It’s also worth remembering how a mass infection strategy was proposed in March 2020 after Peston's Spectator article.
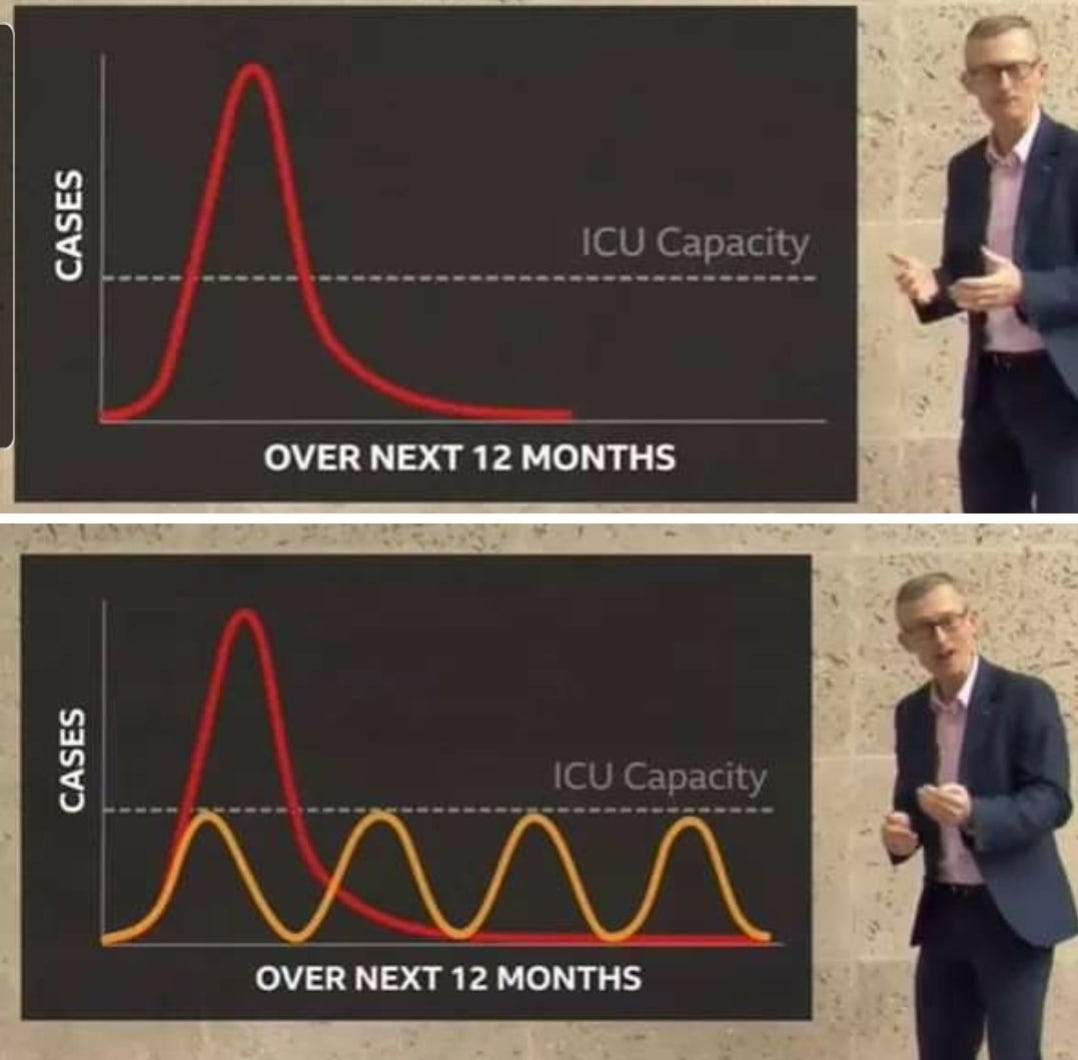
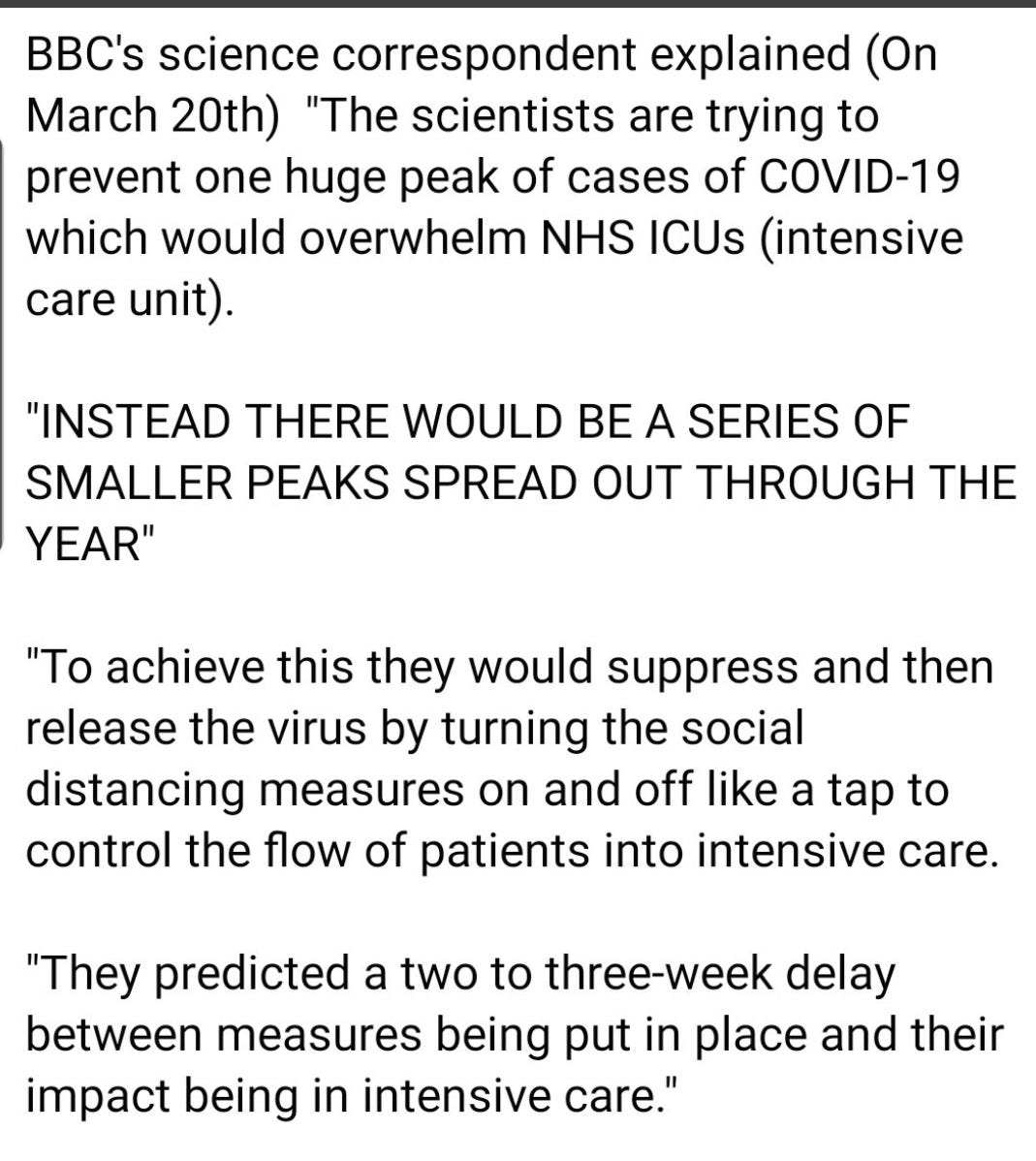
Did the government abandon this plan? Or did it simply struggle to turn the taps the right amount? Winter of 2020 is an example of incremental increases in measures that attempted to level off infection rates rather than rapidly bring them back down.
The Eat Out to Help Out subsidised meal scheme in the Summer of 2020 was said to be designed to stimulate economic activity and also to encourage people to stop the fear as Chancellor Rishi Sunak said. The scheme did lead to increased transmission which would have been welcomed by those supporting a mass infection strategy. Were case numbers considered too low at the start of Summer 2020?
The UKs Covid Inquiry is supposed to have the power to demand evidence, will it use this to determine the motivation behind government decisions making? The public and victims of policy have a right to know if the government followed a mass infection strategy while giving the public misleading information that would increase the risk of infection
Full paper here.

When a patient goes with covid symtpoms to a GP, the first logical thing a medical professional would do is to test the patient for the viral infection suspected, for which a test exists, is cheap and very easy to do. Only that the GPs have no access to covid tests. Where does the fact that most basic & the cheapest step in the fight against covid (covid testing) leave a GP and his/her patient? How is it possible for medical professionals to not have access to tests for a condition that killed millions? What is the justification and what are the real consequences for this? Why does my local hospital's pharmacy has a note in the window to tell us they have no covid tests? What happens when covid is suspected in an outpatient? What is the justification and what are the consequences for this? Why aren't covid tests part of the medical care, in the same way any other tests are? Why aren't covid tests implemented into health care, but left to the patient to decide, not the doctor? Taking tests away from the medical settings has endless consequences for the whole health care system, despite being the simplest, cheapest and most logical step in the fight against covid. There is no logical, financial,economic, humanitarian sense, so why did they do it?
How were doctors trained to acknowledged covid and long covid? Why do the long covid statistics only come from self-diagnosed patients. How many patient, not aware of long covid, are ever diagnosed by doctors? How was covid and long introduced into health care assesments? How can it be introduced into healthcare , when hospitals and GP surgeries don't even wear masks? How did the disinformation campaign affect health care, considering that my local hospitals suddenly gave up masks and used their public health screens to remind patients not to wear maks? At the same time while paediatric wards were getting overwhlemed. Why didn't NHS tell this country that paediatric wards were full in the summer? Why was this mentioned only once at the beginning of winter? Then blamed on lockdowns by the doctors presenting it? How did the disinformation campaing become the norm?