


1.Introduction: Review of the UK's evidence base on Covid in schools
1: Introduction and UK strategy explained

The UK has often been an outlier compared to similar nations, particularly on the issue of schools. The small group of professionals the UK government has relied on to curate its evidence base have become some of the most widely cited researchers of the pandemic, quoted by authorities around the world to justify the removal of measures intended to cut transmission.
Current thinking by high profile people within UKHSA appears to be
Total infections per wave are fixed by the number of susceptibles
Measures merely prolong a wave, cutting transmission in one place will displace the transmission to another location, this argument has been made against investing in clean air in classrooms, if children aren’t infected in large numbers to reach short term herd immunity to end each wave then there will be more infections in care homes and other vulnerable groups
There is no reliable evidence to disprove points 1 and 2
Infections are roughly equivalent to a dose of vaccine for providing immunity, particularly in younger age groups
Infections in younger children are benign enough that there is no need to vaccinate them,
Multiple regular reinfections top up immunity and reduce the risk of severe disease, repeat reinfections will not result in worsening outcomes for the majority, this means that younger children will never need to be vaccinated as regular exposure in childhood will lead to robust protection in adulthood
People will only catch covid around once per 8-12 months, they will not catch it twice in the same wave
Covid won’t throw up any more big surprises
Cumulative health and economic costs of long covid will be sustainable for the workforce, healthcare and the economy
90% of child infections occur outside of schools, transmission reflects community rates
No evidence masks reduce transmission in schools
No evidence ventilation and air filters reduce transmission
Testing for covid causes more disruption than covid infections
Long covid in children is rare, most cases are psychological
Most child deaths from covid are in unhealthy children who would likely have died from another infection if they had been protected from covid
This dominant thinking is exemplified by the decision to end primary vaccination and to only offer boosters to the over 75’s and people with conditions from a narrow definition of high risk.

How did we get here?
Initially at the start of March the public were told that closing schools could be counter productive as it could slow the spread of transmission and reduce the build up of immunity. This was at the start of March 2020 when the UK openly embarked on a herd immunity strategy before U-turning when it became clear the NHS couldn’t withstand the hospitalisation rate, then the government denied herd immunity had ever been the strategy.
A recently published academic paper found that the controversial herd immunity strategy was not properly scrutinised by broadcast media.


As soon as lockdown was declared a media campaign promoting herd immunity launchef the profiles of a number of lockdown sceptic professionals and organisations.
UK Strategy Explained
A April 2020 leaked recording the stark difference between official messaging and what was being discussed behind the scenes.


While Johnson was telling the media the UK would beat the virus in 12 weeks, inside government they were planning for successive waves over years.
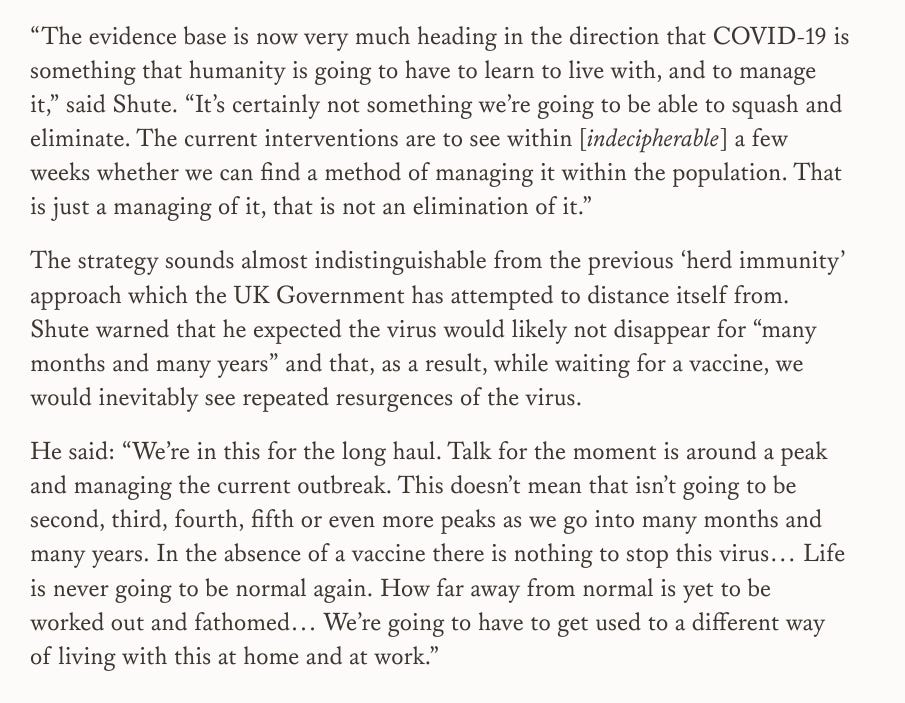
The aim was to stop the NHS from collapsing while keeping as much of the economy open as possible.
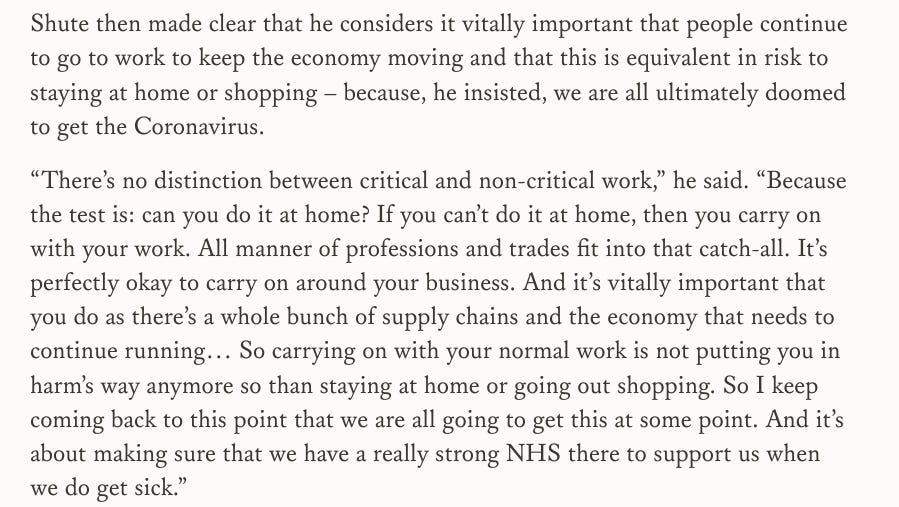
This approach made schools a pivotal part of the pandemic response. Children needed to be in school so parents could go to work, and there was no point in putting measures in place if the expectation was that everyone would be infected before a vaccine was developed.
Conveniently for government strategy, after believing schools would play an important role in building up immunity their advisors then produced evidence that claimed children and schools would actually play no significant role in transmission.
The BMJ's covid inquiry series paper on UK schools policy concluded,

Those responsible for the UK’s evidence base complained that they weren't allowed to mark their homework and organised a rapid response from allies. The response recieved more media attention than the actually BMJ paper, however at best the response could be described as lacking reliability, at worst lacking integrity.
Two threads examining the details of the response.




There is also the issue of confused messaging over airborne vs droplet transmission leading to a focus on hygiene theatre rather than clean air.
There was the WHO's infamous U-Turn.




Minutes from 5 March 2020 from CDC meeting with Canadian Public Health attending shows authorities understood airborne transmission but rather than provide clarity to the public they fudged the messaging with talk of droplets.

The UK will have also known the airborne nature of covid. Authorities in the West chose to confuse the messaging, which wasn't the case in many Asian countries like Japan, South Korea and Singapore.
This had major ramifications for schools leading to nonsensical guidance that was ridiculed by safety campaigners and sceptics alike.
Examining the evidence
This is the first part in a series which will cover the development of the evidence base the UK has relied on from schools guidance to the JCVI.
The series will examine the papers that shaped policy and produced headlines such as “children are 40% less infectious”, “no evidence of a child infecting an adult”, and “only one teacher has died from covid”, it will consider why so little had been done to acknowledge and support long covid children by those who are supposed to protect children, and how concepts like immunity debt suddenly appeared as established fact without an evidence base to support it.